Healthcare Mobile App Development: What It Really Takes to Ship
 Melissa AshfordCOO
Melissa AshfordCOO
Here's the pattern I see over and over: a team builds a healthcare app like it's a consumer app that happens to have a stethoscope on the icon. Then the first real patient record hits the database, and everything they assumed quietly breaks.
It isn't a consumer app. The moment your product touches a real patient record, a clinician's workflow, or a claim some regulator can pull up two years later, the whole thing changes shape. Data model. Logging. Integrations. Timeline. All of it moves at once.
I've watched that bill come due more than once — usually around month four, when someone finally admits the "quick MVP" has to be partly rebuilt. So here's the version I wish more founders got before they signed anything: what actually matters when you build a healthcare app in 2026, where the money leaks out without anyone noticing, and which calls you genuinely cannot walk back later.
Start with the rules, not the screens
Almost every blown healthcare budget I've seen traces back to one habit — design the screens first, treat compliance as something you'll "add later." You can't add it later. By the time the wireframes are signed off, the data model is already wrong, the logging is already wrong, and a good chunk of your integrations are sitting on assumptions that won't survive an audit.
Three questions set the shape of the whole project. Write the answers down — actually down, in a doc — before anyone estimates a single sprint.
Whose data is this, really? Identifiable patient info for US users puts you squarely in HIPAA. EU users bring GDPR, plus MDR the second the app makes a clinical claim.
Does it make a medical claim? "Track your steps" is wellness. "Detect atrial fibrillation" is a medical device. That's not a marketing nuance — it's the line between shipping next quarter and budgeting a multi-month FDA clearance (US) or CE/MDR mark (EU) from day one.
Who are you integrating with? Epic, Cerner, a lab, a pharmacy, a wearable — each one shows up with its own auth, its own data format (FHIR, HL7, take your pick), its own rate limits. Not one of them is a weekend job. I've never seen one that was.
Skip these and you're not saving time. You're borrowing it, at a genuinely ugly interest rate.
 Compliance lives in the architecture long before it ever shows up in the UI.
Compliance lives in the architecture long before it ever shows up in the UI.
The architecture calls that age badly
Where the data physically sits. Encrypt at rest, encrypt in transit — fine, everyone knows that part. The part that actually bites is residency: you have to control where the records live, and prove it on demand. A generic cloud setup that quietly scatters data across regions will fail an audit, and bolting on a dedicated, access-logged layer after launch isn't a patch — it's a rewrite. Build it first.
Audit logging isn't a debug tool here. In a normal app, logs help you chase a bug on a Tuesday afternoon. In healthcare, every read and write of patient data might need to be reconstructable years later. So the audit trail has to live inside your data-access layer from the first commit — not get sprinkled across controllers the week an auditor finally emails you.
Offline is a decision you make on purpose. Clinicians work in basements. Ambulances. Rural clinics running on one bar of signal. If your app quietly assumes a live connection, it'll fold in the exact moments that matter most — and retrofitting offline-first sync after launch is one of the nastiest jobs in all of mobile. Ask anyone who's lived through it.
React Native or native? What we actually reach for
For most healthcare apps we take on, a cross-platform stack — React Native, usually — is the right starting point. One team, one codebase, both platforms. That matters more than usual here, because every change has to be re-validated against your compliance surface, and doing that twice is how schedules quietly die. We only drop to native where there's a real reason for it: secure biometric auth, Bluetooth pairing with a medical device, heavy on-device processing. That hybrid line has shipped real production apps for us without paying the double-codebase tax. So when someone tells a regulated team to maintain two native apps "for performance" before they've proven they need it — I'll push back, and push back hard.
 Healthcare timelines blow up when you price the app and quietly forget the compliance around it.
Healthcare timelines blow up when you price the app and quietly forget the compliance around it.
A timeline that survives contact with reality
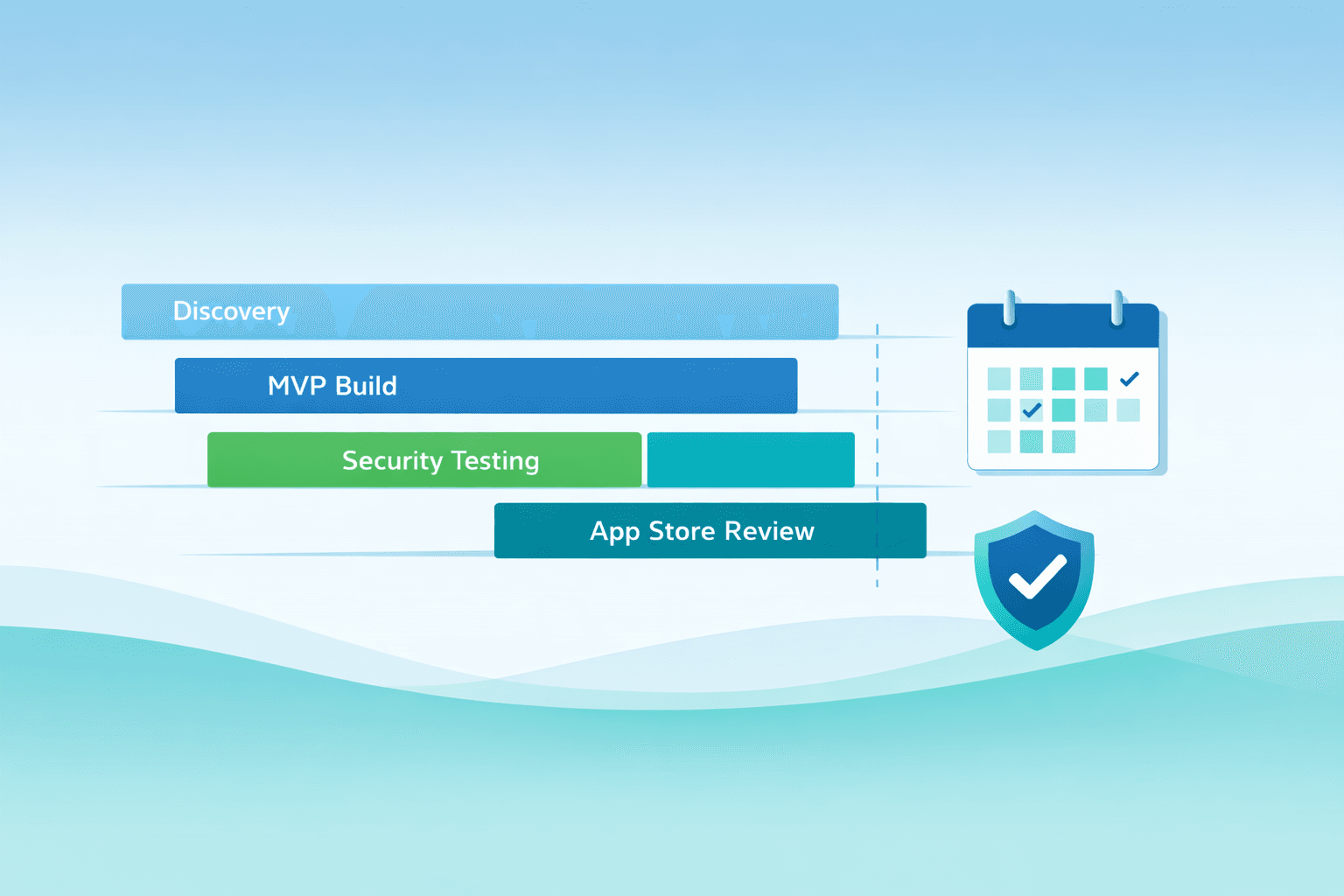
Founders lowball healthcare timelines almost every time, and the reason is dull but consistent: they price the code and forget the compliance wrapped around it. Here's a rough, honest shape for a first version.
Discovery and compliance scoping runs three to five weeks — regulatory surface, data model, the integration contracts. The core MVP build is twelve to twenty, depending on how many systems you have to talk to. Security review and validation adds another three to six, and it should run alongside the build, not wait politely at the end. Then store review — and both Apple and Google lean on health apps harder than just about any other category, so leave room for a couple of extra rounds there.
See "a fully HIPAA-compliant app in six weeks flat" on a quote? That isn't a sharp price. It's a flag.
Where the budget actually goes
The code is rarely the priciest line item. The money pours into integrations — one EHR connection can swallow weeks on its own — plus the security infrastructure and the validation-and-documentation that compliance demands. A cheap quote that skips those isn't cheaper; it just shoves the cost into a worse week, usually the one right before launch, when you have the least room to absorb it. We'd rather put the awkward numbers on the table on day one and have the uncomfortable conversation early than spring a far worse one on you in month five.
 The real gap is between a team that has read about healthcare compliance and one that has shipped through it.
The real gap is between a team that has read about healthcare compliance and one that has shipped through it.
What shipping regulated work actually teaches you
There's a genuine gap between a team that's read about healthcare compliance and one that's been bloodied by it — data residency, audit logging, the medical-claim line, the store reviews that bounce you twice for reasons the rejection email never quite spells out. We've hit those walls ourselves, on real projects, which is exactly why our estimates tend to look different from a generic agency's. Ours are built backward from the audit, not forward from the wireframe. Less fun to present in a pitch. A lot more accurate in month six.
Ready to scope your healthcare app?
If you're weighing one, the most valuable first move isn't a quote — it's a compliance-aware discovery session that tells you what you're actually signing up for. That's where we start with every healthcare client, and honestly, it's the cheapest insurance you'll buy on the entire build.
Talk to the Lomray team about your healthcare app — we'll map the regulatory surface and hand you a realistic plan before you commit a dollar to the build.